Not all pain is the same. That sounds obvious, but it is one of the most common reasons treatment fails. A tendon overload problem is not the same as a nerve compression problem. A fresh ankle sprain is not the same as long-term widespread pain. A stiff joint is not the same as a sensitised nervous system. If the pain type is misunderstood, the plan often becomes too generic.
Understanding pain types helps you ask better questions: Is the tissue irritated? Is a nerve involved? Is this an acute flare-up? Has pain become persistent? Does the plan need strengthening, pacing, medical review, nerve assessment, or education?
Nociceptive pain

Nociceptive pain comes from tissues that are irritated, loaded, inflamed, or injured. This can include muscles, joints, ligaments, tendons, bones, and other tissues.
Common examples:
- Ankle sprain
- Muscle strain
- Tendon overload
- Joint irritation
Also note: Post-operative tissue healing; Mechanical back or neck pain.
Clues include:
- Pain linked clearly to load or movement
- Local tenderness
- Symptoms that improve when the tissue is unloaded
- A clear injury or activity spike
- Pain that changes as healing or loading changes
Treatment often focuses on load management, mobility, strength, and gradual return to activity.
Neuropathic pain
Neuropathic pain comes from irritation, compression, or dysfunction of the nervous system. It often feels different from muscle or joint pain.
Clues include:
- Burning
- Tingling
- Electric shocks
- Numbness
Also note: Pins and needles; Weakness or clumsiness; Symptoms following a nerve distribution.
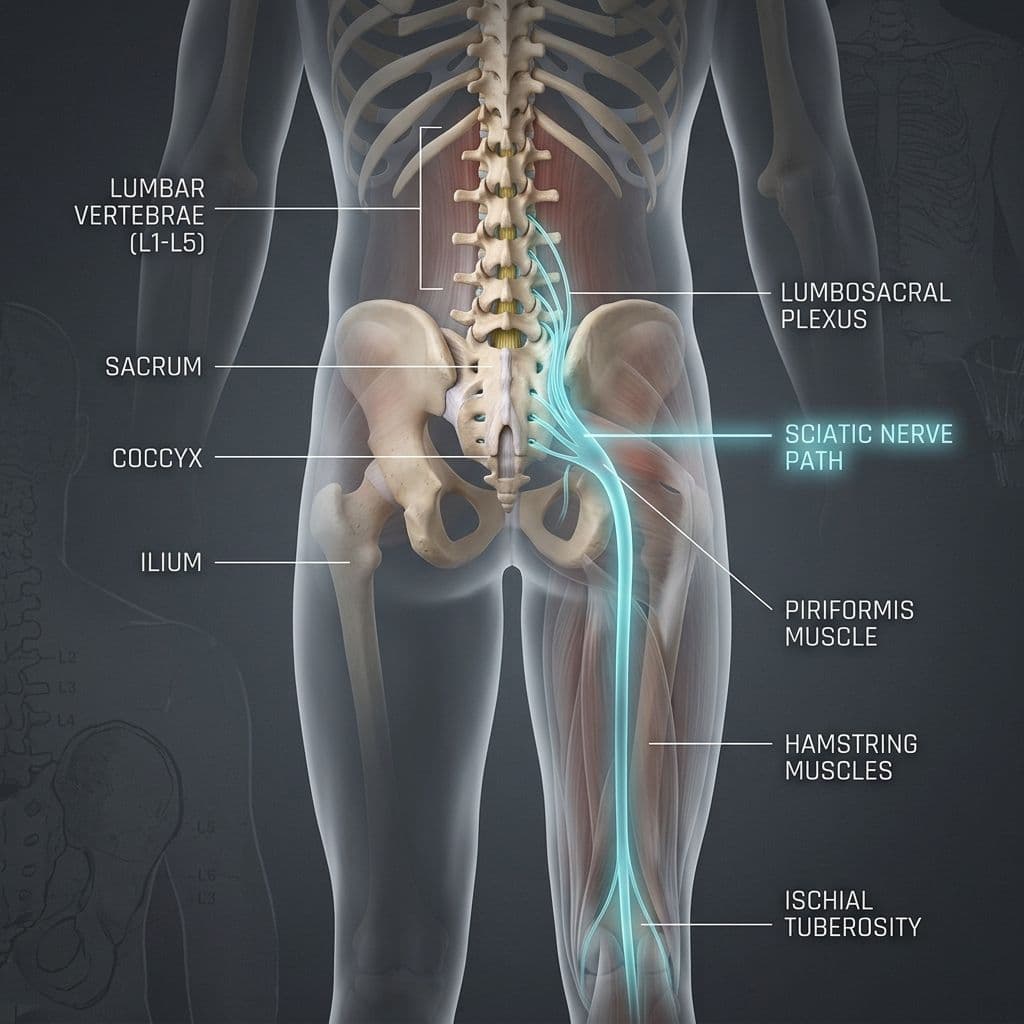
Examples include carpal tunnel syndrome, cubital tunnel syndrome, sciatica with nerve involvement, diabetic neuropathy, and some post-surgical nerve symptoms.
Treatment may include movement modification, nerve-sensitive loading, posture or position changes, strength work, medical review, and sometimes medication or procedures depending on severity.
Acute pain
Acute pain is recent pain. It usually has a clearer trigger and often plays a protective role. If you twist your ankle, acute pain helps you reduce load while the tissue settles. Acute pain is not bad. It is part of the body's warning system.
The rehab goal is to protect the area enough for recovery but not so much that stiffness, fear, and weakness take over.
Chronic or persistent pain
Persistent pain lasts longer than expected and may become less tied to tissue healing alone. It can involve nervous system sensitivity, fear, reduced activity, poor sleep, stress, and loss of confidence.
Persistent pain is real. It is not imaginary. But it usually needs a broader plan than simply resting the painful area.
Mixed pain is common
Many real cases are mixed. A person with low back pain may have nociceptive joint irritation plus nerve symptoms into the leg. A person with diabetes may have neuropathy plus muscle weakness and balance loss. A shoulder problem may involve tissue irritation plus fear of movement after months of pain.
That is why assessment matters. The question is rarely "Which label is it?" The better question is "Which pain mechanisms are most active right now?"
A self-check for pain type
Ask:
- Does the pain burn, tingle, or feel electric?
- Does it stay local, or travel down a limb?
- Is there numbness or weakness?
- Is it linked to a clear movement or load?
Also note: Did it begin after injury, surgery, or a training spike?; Has it lasted longer than expected?; Does stress, sleep, or fear change it?.
The answers help decide the next step.
Why treatment changes by pain type
For nociceptive pain, the main question is usually load: what is the tissue ready for now, and how do we build capacity?
For neuropathic pain, the main question is nerve behaviour: what positions, movements, or health factors are sensitising the nerve?
For acute pain, the main question is protection plus early recovery: how do we calm symptoms without creating unnecessary avoidance?
For persistent pain, the main question is the whole system: how do we rebuild trust, activity, strength, sleep, and confidence?
Mini decision guide
Use this as a starting point:
- Local pain after a clear activity spike: think tissue load and recovery.
- Burning or tingling that follows a pathway: screen for nerve involvement.
- Recent injury with swelling or bruising: protect, assess, and reload gradually.
- Pain lasting months with fear and reduced activity: include pacing and pain education.
- Pain with fever, unexplained weight loss, major trauma, or neurological change: seek medical review.
This guide does not replace assessment, but it stops all pain from being treated the same way.
Why mixed pain needs better planning
Mixed pain is where many people get stuck. A person with sciatica-like symptoms may need both nerve-sensitive positioning and trunk strengthening. A person with knee arthritis may have nociceptive joint pain plus fear of stairs. A person with long-term shoulder pain may have tissue sensitivity plus protective guarding.
If only one part is treated, progress is limited. That is why a full plan may include:
- Symptom education
- Load management
- Strength progression
- Mobility work
Also note: Nerve screening; Sleep and stress discussion; Return-to-activity planning.
The treatment is not more complicated for the sake of it. It is more accurate.
How to track your pain type
For one week, note:
- Location
- Quality of pain
- Trigger
- Duration
Also note: What helped; Whether symptoms travelled; Whether strength or sensation changed.
Bring that pattern to your clinician. It often gives more useful information than simply saying "it hurts."
Examples of matching treatment to type
If a runner develops local Achilles tendon pain after increasing hills, the plan may focus on calf strength, running load, and tendon capacity. If an office worker has tingling into the thumb and index finger at night, the plan may focus on median nerve irritation, wrist position, and carpal tunnel screening. If a person has widespread pain for years with poor sleep and fear of movement, the plan may include pacing, education, graded strengthening, and medical coordination.
Same word, different mechanism. That is why "pain relief" alone is not a complete plan.
What patients can do before the appointment
Prepare useful information:
- Where exactly is the pain?
- What does it feel like?
- What triggers it?
- What eases it?
Also note: How long does it last?; Does it affect strength, sensation, sleep, or confidence?; What have you stopped doing because of it?.
This helps the clinician identify the likely pain type faster and choose a more relevant plan.
Why behaviour matters as much as the label
Patients often want one exact diagnosis, and sometimes that label is available. But pain behaviour is just as important. Does it warm up? Does it worsen after load? Does it travel? Does it wake you? Does it respond to position? Two people can have the same diagnosis but need different plans because their symptoms behave differently. Good treatment follows behaviour, not just terminology.
A useful way to prepare for assessment is to describe the pattern rather than only the pain score. Note where the pain starts, whether it travels, what changes it, how it behaves the next morning, and whether there are nerve symptoms such as tingling, numbness, burning, or weakness. This helps the clinician decide whether the main driver looks more tissue-related, nerve-related, sensitivity-related, or mixed. The goal is not to attach a dramatic label. It is to choose the safest next step and avoid exercises that do not match the pain mechanism.
Red flags
Seek medical review if there is:
- Progressive weakness
- Severe or spreading numbness
- Bowel or bladder change
- Fever, unexplained weight loss, or feeling very unwell
- Pain after major trauma
- Severe night pain that is worsening
- A hot swollen joint
Common questions about pain types
Can I have more than one pain type?
Yes. Mixed pain is common, and treatment should reflect that.
Is nerve pain more serious?
Not always, but progressive weakness, constant numbness, or worsening symptoms should be checked.
Is chronic pain permanent?
Not necessarily. Persistent pain can improve with the right combination of education, pacing, strengthening, medical care, and lifestyle support.
How does physiotherapy decide the type?
Through history, movement testing, strength testing, neurological screening, symptom behaviour, and response to loading.
When unclear pain needs assessment
Book an assessment if you cannot tell what type of pain you have, if symptoms are not improving, or if the advice you are following does not match how your body responds. This is common when pain is mixed. A person may have local tissue pain plus nerve sensitivity, or a healed injury plus persistent protective guarding.
A clinician can test whether symptoms change with load, position, nerve movement, strength demand, or repeated motion. That response helps decide the plan. Without that step, people often collect random exercises and still miss the main driver.
Bring examples of what makes symptoms better and worse. Pain type is often revealed by behaviour over time, not by one isolated test. Your observations can make the assessment sharper.
Explore pain and nerve guides
Clinic takeaway for pain patterns
Pain labels are useful only when they change the plan. At Physynex, we identify the main pain mechanism, explain what it means, and build treatment around the actual pattern rather than a generic exercise sheet.